Motivation
 |
 |
 |
 |
 |
 |
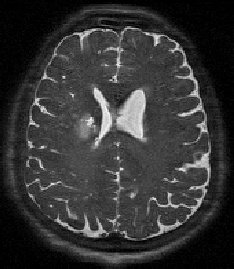
Treatment for stroke requires almost immediate intervention, and quick, consistent computer segmentations would be useful for evaluating alternative therapies.
Automatic segmentation of stroke lesions in magnetic resonance imagery is a difficult problem because anatomical knowledge is required for the most accurate decisions. Without such knowledge, classification rules seem inconsistent.
Creating and evaluating automatic methods for segmenting lesions is challenging for two major reasons. First, the concept of a ground-truth segmentation is elusive because manual segmentations can greatly differ among physicians. Second, as shown above, the images of the lesions themselves vary widely.
We have created a nearly entirely automatic system that requires ony two simple inputs from a user and can match (on average) the volumes given by physicians with a clinically useful variance.
Overview
We overcome the problem of enormous variety by giving the user an easy choice among potential segmentations. After the user selects seed points that give the inside and outside of the lesion, we calculate a edge-preserving multi-scale view of the image. At each scale an implicit three-dimensional active contour (or balloon) is inflated from the inner seed point. Several segmentations are given by varying the edge-finding parameters of the balloon.
After all the segmentations are found, we calculate the frequency of a voxel's inclusion and use this as an estimate of the "confidence" that the voxel is a lesion. The user may then choose the system confidence that gives the segmentation most closely matching their own.
Nonlinear Scale Space
 |
 |
 |
 |
 |
We desire to model the segmentation of lesions in a framework that captures the variety of lesions. So-called scale-space methods blur an image so that details disappear as the scale increases. Our goal is to localize lesion boundaries, so we use the edge-preserving scale-space provided by nonlinear diffusion. Edges are preserved and enhanced by encouraging blurring within regions while restricting blurring between them.
Geometric Deformable Model
 |
 |
 |
 |
 |
For segmenting both complex and regular shapes quite easily, we employ geometric deformable models, or level sets. These require a single click to initialize and inflate like balloons that fill to lesion boundaries. With one additional click by the user, we may find the intensity of normal tissue.
We then use a method that combines intensity and boundary cues to detect lesion boundaries and thus stop inflating the balloon. Our hybrid method allows for multi-modal lesions to be segmented correctly by not relying solely on gradient strength and prevents the ballon from inflating beyond the lesion when there is no strong edge to stop it.
Example Results
 |
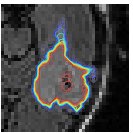 |
Segmenting the image many times, we can count how often particular voxels are labeled as lesion and use this as a measure of confidence. Physicians may then choose which confidence boundary most closely matches their ideal segmentation, without having to draw any boundaries themselves.
| Original |
|---|
 |
| Physician Segmentation |
 |
| Automatic Confidence Boundaries |
 |
In the figure at left, our method allows a user to choose even the lowest confidence contour as the proper segmentation boundary.
Our results show that it is possible to achieve almost zero volume error for each image and each physician. All volume differences are well within clinically useful bounds.
Related Papers
- Nonlinear diffusion scale-space and fast marching level sets for segmentation of MR imagery and volume estimation of stroke lesions, with G. Bissias, E. Riseman, A. Hanson, and J. Horowitz. In Sixth Annual International Conference Medical Image Computing and Computer Assisted Intervention (MICCAI), Nov 2003. [PS.gz] [PDF] [bib] [doi]
- Confidence-based segmentation of MR imagery using region and boundary information with nonlinear scale-space and fast marching level sets, with G. Bissias, E. Riseman, A. Hanson, and J. Horowitz. Technical Report UM-CS-2003-017, University of Massachusetts-Amherst, Amherst, MA 01003-4601, April 2003. [PS.gz] [PDF] [bib]